CAP Today's April cover article focuses on tumor gene panel testing, clinical standards, and continuing reimbursement woes. Also discussed: Standing orders and pathologist orders for genomics.
_____________________
Molecular pathology is always a moving front - NIPS, hereditary gene panels, tumor gene panels, tumor gene panels by-liquid-biopsy, minimal residual disease testing, transcriptomics, multi-cancer early detection - each has its own collection of evidence, guidelines, FDA labeling, its interactions with NCDs or laws, and other factors.
On one of the oldest fronts, hereditary gene panels, recent news again that legacy guidelies and coverage rules miss far too many cases (a "policy-based" false negative, rather than a lab-based one) - here. Meanwhile, in the past year, MolDx has taken the position that it won't pay for BRCA testing alone, it ust be part of a panel (testing alone is both more costly and per MolDx, below a stardard of care that Medicare requireres.) See open access news here. Subscription coverage at Genomeweb here.
On another of the older fronts, tumor gene panels, like the Foundation Medicine test, see a deep-dive article by Karen Titus of CAP TODAY in the April issue. Here.
A wide range of topics are discussed in this article, including the history of the field, the switch to next-gen sequencing, the Medicare NCD in this space, the lack of equity in test availability, and contrasts between what happens major cancer centers and community care.
Also catching my attention, a discussion of standing orders (so no patient gets missed) and pathologist-based ordering. NOT mentioned, but I think relevant, a Medicare law that diagnostic test orders must be made by the patient's treating physician who is directly provider her/his medical care. This is found at 42 CFR 410.32, and I discuss it in an April 2022 blog with some history and further references. Here. Medicare policy manual 15:80.6.4 gives very limited zones for pathologist test orders, such as seeing TB-like specks on a H&E and ordering a TB stain "to complete the case." The CAP TODAY article also brings up direct physician payment to an MD, which occurs for "physician pathology tests" like a lymph node biopsy, but not for genetics. This is related to a regulation that a physician service must be performed by a physician >50% of the time (see 42 CFR 415.130, 415.102(a)). I discussion those links in my April 2022 blog also.
(I also link to an even nerdier 2013 white paper here. The topic also turns out to be tied into historical legal definitions of what services are paid to a hospital (TC) and paid to a physician (PC)).
With regard to lack of payment for genomic interpretation services, Medicare would argue that they pay $3500 for, say, a Foundation Medicine test, out of which the company can pay whatever it chooses to, to either physician lab directors or PhD professionals who are involved signing out in the test.
I haven't been a practicing pathologist since 2000, but reading the article I had half-an-idea there may be two uses of the term Standing Orders. One is per-patient (an order to take the particular patient's glucose every day at 8 am and 8 pm x 7 days), the other is per-protocol (order a Foundation Medicine test on every metastatic cancer this year). Medicare has some rules for the former.
___
Regarding turn around time for cancer sequencing, see a March 24 premium article by Andrew Han at Genomeweb here.
Regarding uninterpretable 30-page genomics reports, see an article by Beauchamp et al. on "integrative diagnostics," here. (There is also a forthcoming paper by MGH on this topic).
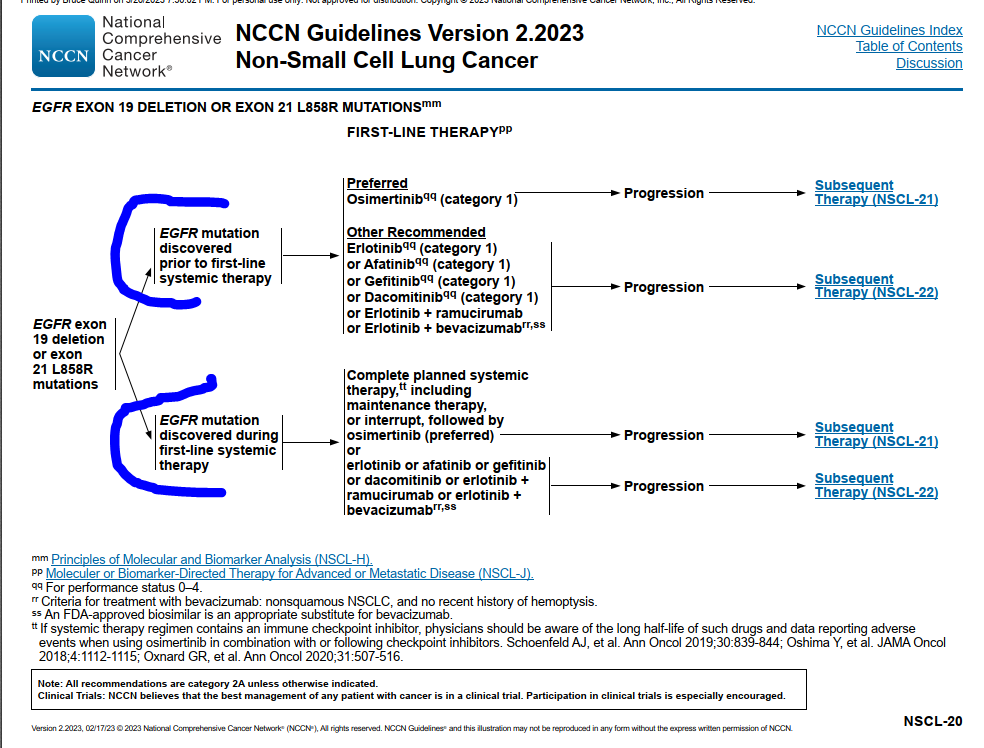
The NCCN Flow Chart for Lung Cancer: We Should Be Appalled, Not Take as Status Quo
Regarding starting chemotherapy in lung cancer before molecular testing is done, there's a silent testimony to this problem baked right into NCCN guidelines. They have flow charts when genomic testing is quirkcly available, and separate flow charts for other patients, specifically when genomic testing is delayed. Having to enshrine that dysfunction in major protocols is sad.
See guideline 2.2023, NSCL-20, with one flow chart if a critical EGFR mutation is discoveried in time for treatment, and another flow chart of the same patient if all too often the discovery of the EGFR mutation is delayed.
 |
| click to enlarge |