We often puzzle over exactly how USPTF decisions are made, or how quality measures are debated, chosen, and implemented by payors. Different stakeholders may take opposite sides for numerous reasons, including perceived economic ones.
An excellent paper by Zhu et al. in Annals of Internal Medicine this month sheds a light on this. If we have to choose, why not bang for the buck, or benefit for the resources, if you prefer. Let's drop the $1000 quality measure that generates $100 of health value, and instead let's pick the $100 quality measure that generates $1000 of health value. Sounds simple, until you realize the status quo is for Specialty X to want measure X, and Specialty Y to want Measure Y, and they argue-and-arm-wrestle to a decision.
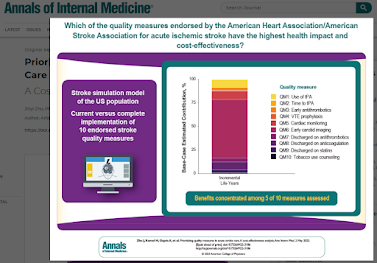
In the field of stroke care, Zhu et al. assert that most of the benefit (impact) was expected to come from just 5 of 15 possible stroke quality measures. Scarily, only 10 of 15 endorsed quality measures had enough outcomes data to allow a cost/benefit analysis. 2 of the 15 measues carried 70% of the value and 5 of the 15 measures carried 90% of the value.
https://www.acpjournals.org/doi/10.7326/M22-3186
The article has an editor's Visual Abstract:
 |
| click to enlarge |
Substantial variation exists in the potential net benefit of quality improvement across AIS quality measures. Benefits were highly concentrated among 5 of 10 measures assessed. Our results can help providers and payers set priorities for quality improvement efforts and value-based payments in AIS care.
_____
More of this kind of work is probably a good thing.
On the same theme: A new Cass Sunstein article on algorithms in public policy - here.
See a USC article on a special sort of cost/benefit analysis called GRACE.

art, bing.com/create