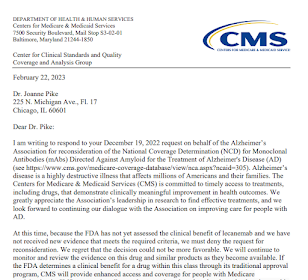
Almost every week, someone reaches out to me about a dispute related to evidence (can Product X be covered, or not covered?) We saw this issue in headlines this week, when CMS publicly declined a request from the Alzheimer's Association to update Medicare's non-coverage of certain disease-modifying drugs in dementia (entry point here.)
At a Medicare meeting this week, a senior medical director remarked that people would like simple numeric rules for evidence (like "How many patients in a trial?") but that it's not that simple. Some smaller trials have big effects (patients live 12 months versus 24 months) and some large studies have minor or confusing small effects. So, it depends on a layer of expert judgement that is contingent on circumstances. More so probably in diagnostics, where the value is dependent on downstream events, like therapy choices. (Emphasized recently in Soares, Establishing the Value of Diagnostic and Prognostic Tests, 2018 here.).
Disputes For Centuries, at High Temperatures
These disputes have gone on for centuries, and debates from the 1500s and 1600s seem surprisingly fresh in tone. In the early 1500s in Italy, Tartaglia and Cardano fought bitterly and publicly, and enlisted enemies and allies, over mathematical proofs (Hellman 2006). William Harvey's theory of circulation of the blood, published 1628 (in Germany; banned in England!) brought hostile debates, and literally one book after another was published to tear Harvey's ideas apart (Hellman 2001).
One of my very favorite quotes about evidence disputes I've seen only in a rare book (Stern, 1941). Late in life, Harvey wrote:
"Scare a day, scarce an hour, has passed since the birthday of of the circulation of the blood that I have not heard something for good or evil said of this discovery. Some abuse it as a feeble infant, and yet unworthy to have seen the light. Others again this the bantling deserves to be cherished and cared for. These oppose it with much ado, those patronize it with abundant commendation. One party holds I have completely demonstrated the circulation of the blood by experiment, observation, and ocular inspection, against all force and array of argument. Another thinks it is scarcely, but sufficiently demonstrated, not yet cleared of all objections..."
Stern writes, "Harvey claimed that no man over forty was found to adopt the doctrine of circulation of the blood," placing Harvey with an idea attributed to Max Planck, that scientific ideas win because their opponents eventually die.
Medical Progress and Leadership
In a new book, biotechnology expert Brian Smith (2022) explains that the life sciences and medical technology are an ecosystem with many parts, and often not well-designed to achieve effective medical progress. Many ecosystems have disparate goals (NIH, biopharma, investors, payors, physicians, patiens, and so on). I was reminded of the role of leadership in these situations by page 1 of a book by Kissinger (2022). Imagine the following paragraph in regards to the health innovation context -- such as CMS National Coverage Determinations, or CMS "Transitional Coverage for New Technologies," or the MolDx molecular test program.
"Any society is perpetually in transit between a past that forms its memory, and a vision of the future that inspires its evolution. Along this route, leadership is indispensible...to help people reach from where they are to where they have never been,and, sometimes, can scarcely imagine going. ...[Leaders] must balance what they know, which is drawn from the past, with what they intuit about the future, which is inherently conjectural and uncertain. It is this intuitive grasp of direction that enables leaders to set objectives and lay down a strategy...communicating objectives and rallying support."
Although I didn't have this quote at that time, it's this thought I had in mind when I wrote that I was disappointed that a recent CMS two-day workshop on "Evidence Development" focused its expert panel on answering only questions about methodology and not where we should be going and why. To me, this is like a focus on how thick the asphalt on a road should be, displacing a chance to focus on to where the road should be built and why. The "methods-only" focus (or any other single-minded focus) there in the payor silo powers the separately-spinning and inefficient medtech ecosystem that Smith (2022) writes about.
###
By the way, in the field of diagnostic testing, the concept of "value" as clinical utility is not new. When I was in medical school in the 1980s, we students were asked, "Why order that test, and how will it impact this patient's care?" And in 1800 when Laennec discovered the stethoscope, one naysayer immediately took the position, "You will learn nothing by it, and, if you do, you cannot treat the disease any better," which is pretty good for a 223-year-old definition of clinical utility from a diagnostic procedure. (Hellman, 2001, p X).
##
Hellman H (2001) Great Feuds in Medicine.
Hellman H (2006) Great Feuds in Mathematics.
Kissinger H (2022) Leadership.
Smith B (2022) Darwin's Medicine: How Business Models in the Life Sciences are Evolving.
Stern B (1941) Society and Medical Progress.
Planck's original quote, 1948 (Gegner allmählich aussterben).